

Between $700 billion and $1.1 trillion every year.
This amounts to between 21% and 34% of the $3.3 trillion total healthcare spending for 2016.
These figures are the estimates published in 25 authoritative studies done between 2003 and 2012. Donald Berwick MD, former head of Medicare, assembled these 25 studies for the RAND Corporation.
Fixing U.S. Healthcare blog has used the terms non-costworthy and low-marginal-benefit for this kind of wasted spending. But whatever the terminology, it adds up to healthcare services that are not worth the money. See my YouTube video on this subject, as well as my previous posts addressing two examples, Repatha (evolocumab) cholesterol drug and Tarceva (erlotinib) 2nd-line chemotherapy drug.
Dr. Berwick’s study is available as an abstract or full article. He also has a short interview about the study on YouTube.
Six Categories of Waste
Dr. Berwick breaks wasted health dollars down into 6 categories (in his own words):
- Failures of Care Delivery: the waste that comes with poor execution or deviation from known best care processes, resulting in patient injuries or poor clinical outcomes. He estimated this category at between $102 billion and $154 billion in wasted spending in 2011.
- Failures of Care Coordination: the waste that comes when patients fall through the slats in fragmented care resulting in complications, hospital readmissions, loss of independence especially for the chronically ill. He estimated this category at between $25 billion and $45 billion in wasteful spending in 2011.
- Overtreatment: the waste that comes from subjecting patients to care that, according to sound science and the patients’ own preferences, cannot help them. Examples include excessive use of antibiotics, use of surgery when watchful waiting is better, and unwanted intensive care at the end of life for patients who prefer hospice and home care. He estimated this category at between $158 billion and $226 billion in wasteful spending in 2011.
- Administrative Complexity: the waste that comes when government, accreditation agencies, insurance payers, and others create inefficient or misguided rules. Examples are non-standard insurance forms and non-interoperative computer systems. He estimated this category at between $107 billion and $389 billion in wasteful spending in 2011.
- Pricing Failures: the waste that comes as prices are higher than would be expected in well-functioning markets, For example, because of monopolies and obfuscated billing, US prices for diagnostic procedures such as MRI and CT scans are several times more than identical procedures in other countries. He estimated this category at between $84 billion and $178 billion in wasteful spending in 2011.
- Fraud and Abuse: the waste that comes as fraudsters issue fake bills and run scams, as well as the cost of policing. He estimated this category at between $82 billion and $272 billion in wasteful spending in 2011.
Here is a cost-benefit graph representing waste in economic terms as “low-marginal benefit” service purchases.
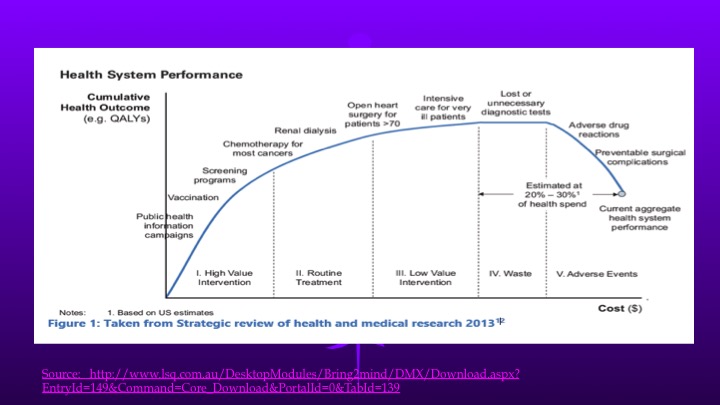
See my previous post for more explanation of low-marginal-benefit services. This graph depicts the effects of overtreatment, failures of treatment, and poor coordination. Administrative complexity, overpricing and fraud-and-abuse depress this cost-benefit curve further across the whole span of marginal costs, according to Dr. Berwick’s model.
Dr. Berwick’s article urges all healthcare stakeholders to work on all 6 categories to eliminate wasted healthcare spending and thereby achieve zero-growth in its percentage of GDP.
Dr. Berwick on Cost-Benefit Analysis
Dr. Berwick is on record elsewhere as favoring cost-benefit analysis such as used by Britain’s National Health Service to evaluate costworthiness of new drugs and technologies.
I note that this approach is similar in concept to that used by the Oregon Health Plan of 1994. By eliminating Medicaid payment for the least costworthy services, Oregon addressed overtreatment and pricing directly, and all of the other factors indirectly. Oregon also used managed care to improve care coordination. See more details.
Thus, an Oregon-type approach would address all 6 categories of wasted spending.
More Wisdom from Dr. Berwick
Dr. Berwick cautioned (in his own words):
- Waste reduction will require focused leadership, with bold and explicit goals, honest monitoring, and strong cooperation between public and private payers.
- Rooting out waste will also require commitment from health care professions, who can most accurately tell the difference between waste and what helps.
- However, extracting even a small fraction of the total waste from an industry that represents nearly one-fifth of the US economy still poses a major threat of economic disruption. Long-range US health care reform will require sound and respectful pathways of transition from business models addicted to doing more and more to ones that do only what really helps.
- To that end, Dr. Berwick advocates setting a target to keep healthcare spending at current levels – zero growth with no winners or losers — at least for the time being. The GDP-percent target put forth in his article was 17.6%, the 2011 statistic; healthcare’s percent of GDP for 2016 is now 17.9%.
- Obtaining savings directly—by simply lowering payments or paying for fewer services—seems at first glance like an obvious remedy. But eliminating waste is a better strategy for rebuilding a health system that is affordable, sustainable and effective for delivering truly beneficial care for all Americans.
Now, take action
Graphic credit: Australian Dept of Health & Aging – Strategic Review of Health and Medical Research, February 2013 http://www.lsq.com.au/DesktopModules/Bring2mind/DMX/Download.aspx?EntryId=149&Command=Core_Download&PortalId=0&TabId=139
Photo Credit: This is an image of Donald Berwick, who was the Administrator for the US Federal Center for Medicare and Medicaid Services (CMS). CMS is part of the US Department of Health and Human Services. The source website is federally managed by the Department of Health and Human Services. This image is a work of the United States Department of Health and Human Services, taken or made as part of that person’s official duties. As a work of the U.S. federal government, the image is in the public domain.

16 thoughts on “FAQ: How Many Healthcare Dollars Are Wasted?”