
Financial pollution arises when exorbitant or unnecessary healthcare spending depletes resources needed for the wellbeing of the population. This is the subject of a JAMA Health Forum Insight co-authored by researchers in the Department of Population Medicine at Harvard Pilgrim Health Care Institute and Harvard Medical School. The Insight was published in the March 8, 2021 issue […]U.S. … Continue reading U.S. healthcare system full of ‘financial pollution’ — Scientific Inquirer re-blog
Category: Healthcare Waste
Slow Vaccination Is a Tell-Tale Symptom of a Sick Healthcare System
Might the U.S. have improved its COVID-19 vaccination roll-out by having a Medicare-for-all single-payer system in place? The simple answer is, You betcha! The three main problems with the United States vaccination effort are lack of centralized control, fragmented delivery systems, and non-interoperable data systems for tracking. Local healthcare monopolies can be “free-lancers,” operating willy-nilly … Continue reading Slow Vaccination Is a Tell-Tale Symptom of a Sick Healthcare System
Medicare for All Requires Healthcare Delivery Reform
I am happy to re-blog this post entitled, Medicare for All Requires Healthcare Delivery Reform, below. This post was offered by fellow blogger Ken Terry, who has been a respected health economics journalist for decades. I add comments about points of agreement, some other valid insights, alternative points of emphasis, and questions, posed somewhat rhetorically. … Continue reading Medicare for All Requires Healthcare Delivery Reform
Fixing U.S. Healthcare – Annual Review & Summary
Fixing U.S. Healthcare blog’s two-year anniversary is a good time to take stock of what has changed in our approach to fixing U.S. healthcare. And a good time to review highlights of the last year. Elevator Pitch for Fixing U.S. Healthcare Let’s start with an “elevator pitch” summary: The U.S. healthcare system has outgrown itself, … Continue reading Fixing U.S. Healthcare – Annual Review & Summary
AMA Journal Blames Greed and Politics for Rising Healthcare Costs
A new study in the Journal of the AMA (JAMA) finds that 25% of the current $3.5 trillion spent by Americans on healthcare is wasted – dollars spent that don’t help achieve health or relieve disease.
Fellow blogger Henry Kotula has summarized the findings, as re-posted below.
Commentators on the JAMA article echo Fixing U.S. Healthcare blog’s messages:
• Exorbitant healthcare spending diverts resources from “the nation’s schools, small businesses, road builders, bridge builders, scientists, individuals with low income, middle-class people, would-be entrepreneurs, and communities as a whole [which] could make much, much better use of that money.”
• The largest cost drivers are administrative fragmentation ($265 billion) and bloated prices ($240 billion). Note: The JAMA study also identified low-value care as a driver, but only looks at three categories: over-aggressive terminal care, misuse of testing, and over-use of brand-name drugs. Fixing U.S. Healthcare blog has claimed that low-benefit-high-cost care is a more pervasive and significant cost-driver.
• The JAMA article shows that up to $282 billion could be saved simply by implementing at scale measures that have already been proven
• However, interventions so far have been piecemeal and haphazard
• Monopolies in healthcare are a key driver of cost
• Many interventions save money at first pass, but then result in cost-shifting (“squeezing balloons”)
• While healthcare costs are an increasingly obvious issue in the United States, they are also emerging as an issue in other advanced countriesGreed & Politics Are the Root Cause
Beyond these findings, the most incisive accompanying editorial by Don Berwick MD, MPP, who was featured in our previous post, points out that what these researchers call “waste” others in the healthcare sector call “income.” He further observes thatWhen big money in the status quo makes the rules, removing waste translates into losing elections. The hesitation is bipartisan. For officeholders and office seekers in any party, it is simply not worth the political risk to try to dislodge even a substantial percentage of the $1 trillion of opportunity for reinvestment that lies captive in the health care of today.
So, he concludes,
the challenge of removing waste from US health care and reinvesting that harvest where it could do much more good is not a technical one. It is a political one. In short, removing waste from US health care will require both awakening a sleepy status quo and shifting power to wrest it from the grip of greed.
None of the researchers or editorialists came right out and said it. But we do know where waste lies. And we know how to root it out. And that will happen only when Americans awaken and when they collectively, through the only institution powerful enough to overcome that greed and politics – the U.S. government – demand fixing U.S. healthcare. And only when all agree to be part of that fix.
Enjoy the summary, below.
Now, Take Action.
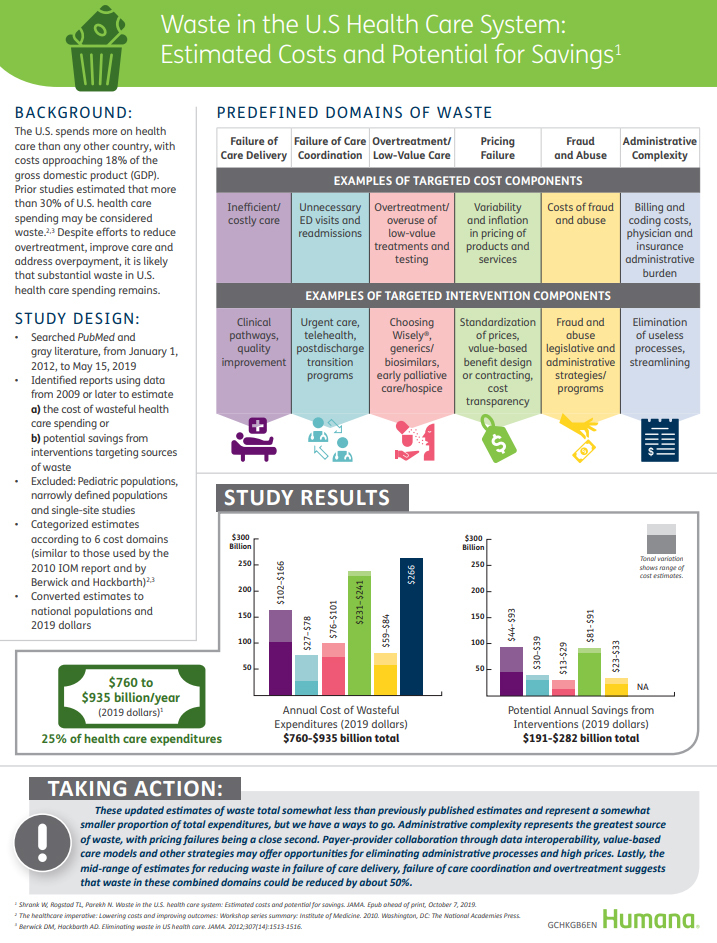
About 25 percent of U.S. healthcare spending can be classified as waste, according to a new study published in JAMA Oct. 7.
For the study, researchers from Humana and the University of Pittsburgh School of Medicine analyzed 54 peer-reviewed studies, government reports and other medical literature to estimate the levels of waste in the U.S. healthcare system.
Researchers divided waste into six previously developed categories including: failure of care delivery; failure of care coordination; overtreatment or low-value care; pricing failure; fraud and waste; and administrative complexity.
Administrative complexity accounted for the most waste with $265.6 billion annually, followed by pricing failure or inefficiencies, which accounted for up to $240.6 billion in waste per year.
Approximately $300 billion in waste accrued from failure of care delivery, failure of care coordination and overtreatment. The study estimated that about half of this waste could be avoided.
Overall, the researchers found that the…
View original post 51 more words
